

Introduction: Thrombotic thrombocytopenic purpura (TTP) is a life-threatening thrombotic microangiopathy (TMA) resulting from severe ADAMTS13 deficiency, which is generally treated with therapeutic plasma exchange (PLEX). Although ADAMTS13 activity is often assayed to differentiate TTP from TMAs not requiring PLEX, technical and logistical constraints often limit rapid turnaround of results, with PLEX initiated based on clinical suspicion of TTP while awaiting ADAMTS13 activity results. We estimated the potential reduction in plasma product use if rapid turnaround ADAMTS13 activity testing were available in our centre.
Methods: We reviewed medical records for all Vancouver General Hospital patients with ADAMTS13 activity testing since assay implementation. Patients receiving PLEX but ultimately diagnosed with a disease not requiring PLEX were identified as "potentially avoidable PLEX" (paPLEX), and their plasma product exposures and related blood product costs were estimated. Laboratory results, ADAMTS13 activity, and PLASMIC scores (a validated clinical tool for TTP diagnosis) of this group were compared to those of newly diagnosed TTP patients (N=35).
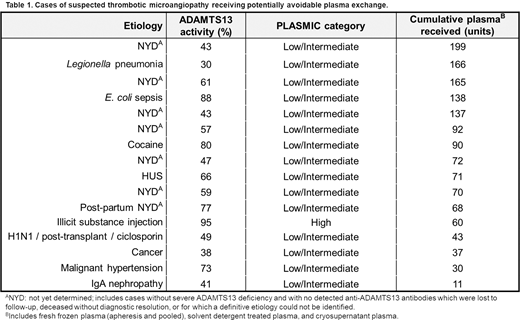
Results: We identified 16 paPLEX patients, including TMAs secondary to malignant hypertension, infection, hemolytic uremic syndrome, illicit drug use, autoimmune renal disease, and malignancy (Table 1). These patients underwent 104 total PLEX cycles (3-12 per patient, median 6), involving 1,428 plasma units (28-199 per patient, median 71.5) and estimated product-associated costs of $187,759 CAD ($140,889 USD). Median platelet counts were significantly lower in TTP than the paPLEX group (7x109/L versus 38x109/L), as was serum creatinine (98µmol/L versus 224µmol/L). PLASMIC scores indicating low or intermediate likelihood of TTP were observed in 63% of patients receiving paPLEX and 17% of patients with TTP. All patients with TTP had ADAMTS13 activity < 10%, while all patients receiving paPLEX had ADAMTS13 activity ≥ 30%.
Conclusions: Unnecessary PLEX carries significant patient blood product exposure risks and system costs that may be circumvented if TTP can be reliably distinguished from other TMAs at the time of initial presentation. In our cohort, ADAMTS13 activity results provided clear separation of these groups and improved upon TTP diagnosis by clinical judgement and PLASMIC scores. Rapid turnaround of ADAMTS13 activity testing results has the potential to reduce the unnecessary costs and blood product exposures resulting from PLEX administration to patients with non-TTP TMAs.
Smith:Alexion: Other: Participated in an advisory board without receiving financial compensation.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal